|
| Zurück |
Dietary Supplementation
With the Tribomechanically
Activated Zeolite Clinoptilolite
in Immunodeficiency: Effects
on the Immune System
Slavko Ivkovic, MD
Zagreb, Croatia
Ulrich Deutsch, MD
Negast, Germany
Angelika Silberbach, MD
Richtenberg, Germany
Erwin Walraph, MD
Laboratory for Immunology
Neubrandenburg, Germany
Marcus Mannel, MD
Ad libitum Medical Services
Berlin, Germany
ABSTRACT
Natural zeolites are crystalline aluminosilicates with unique adsorption, cationexchange, and catalytic properties that have multiple uses in industry and agriculture. TMAZ®, a natural zeolite clinoptilolite with enhanced physicochemical properties, is the basis of the dietary supplements Megamin® and Lycopenomin®, which have demonstrated antioxidant activity in humans. The aim of this prospective, open, and controlled parallel-group study was to investigate the effects of supplementation with TMAZ on the cellular immune system in patients undergoing treatment for immunodeficiency disorder. A total of 61 patients were administered daily TMAZ doses of 1.2 g (Lycopenomin) and 3.6 g (Megamin) for 6 to 8 weeks, during which the patients' primary medical therapy was continued unchanged. Blood and lymphocyte counts were performed at baseline and at the end of the study. Blood count parameters were not relevantly affected in either of the two treatment groups. Megamin administration resulted in significantly increased CD4+, CD19+, and HLA-DR+ lymphocyte counts and a significantly decreased CD56+ cell count. Lycopenomin was associated with an increased CD3+ cell count and a decreased CD56+ lymphocyte count. No adverse reactions to the treatments were observed.
Keywords: zeolites; clinoptilolite; TMAZ; dietary supplements; clinical trial; immunologic deficiency syndromes; immunomodulators; immunotherapies; superantigens; antioxidants INTRODUCTION
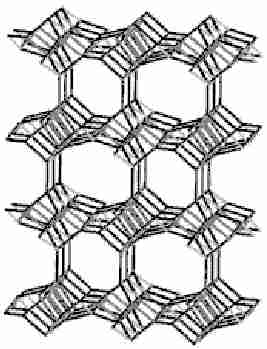
Zeolites are natural minerals of volcanic origin that can be characterized as crystalline hydrated aluminosilicates of alkali and alkaline earth cations having an infinite and open three-dimensional structure (Fig 1). The ability of zeolites to lose and gain water reversibly and to exchange extra-framework cations, both without change to the crystalline structure, is the basis of their unique properties as "molecular sieves." Zeolites exhibit versatile adsorptive, cation-exchanging, dehydrating-rehydrating, and catalytic properties that make them suitable for multiple uses in industry and agriculture. Specifically, they are used to dry acid gases; separate oxygen from air; remove NH3 from drinking water and municipal wastewater; extract cesium and strontium from nuclear wastes; deodorize animal litter, household items, and clothing; serve as soilless zeoponic substrates for greenhouses and space missions; and supplement swine and poultry feed.1
Fig 1. Crystal structure of the zeolite clinoptilolite with its 8-ring and 10-ring channels.When ingested, powdered zeolites, like almost all silicates, are inert and therefore do not react chemically with food or body fluids or their metabolites. The risk of any associated adverse effects is therefore insignificant. In toxicology studies involving mice and rats, the administration of the zeolite clinoptilolite during a period between 6 and 12 months caused no changes that could be considered a toxic effect of treatment.2
Zeolites have also been investigated in a broad spectrum of medical uses. Several of these applications take advantage of the adsorption and ion exchange properties of zeolites. A urease-zeolite preparation is administered in oral microcapsules, for example, to remove urea from the blood in patients with uremia.3 Zeolites are also used as a filter medium for exchanging NH4 + during hemodialysis and hemoperfusion.4,5 They are also used as an antidiarrheic drug.6 Among the zeolites that have shown promise in medical applications, Na2CO3-clinoptilolite has proved to be an effective and safe antacid for patients with ulcer disease,1,2 and gadolinium zeolite has proved useful as a contrast medium that enhances the imaging of the gastrointestinal tract during magnetic resonance imaging.7 In vitro studies of the synthetic zeolite A revealed the mineral induces the proliferation and differentiation of osteoblast cells and the activation of osteoblast cell function, findings that suggest zeolites may have therapeutic properties in the treatment of osteoporosis.8 Recently, two clinical studies involving healthy volunteers and patients suffering from malignant disease and diabetes demonstrated that orally administered natural clinoptilolite is a potent antioxidant.9, 10 When applied externally in powder form, zeolite has also been found to quicken the healing of wounds and surgical incisions; in Cuba, clinoptilolite is commonly used to treat topical wounds in horses and livestock.1 As proven bactericides and fungicides, zeolites have been used to control urinary tract infection and dental plaque formation.11-13 It is well known that silica particles prevent almost completely the onset of spontaneous diabetes in young BB rats and the destruction of β cells in nonobese mice given cyclophosphamide.14, 15 In mice with alloxan-induced diabetes, natural clinoptilolite has been shown to avert or diminish some late sequelae of the disorder, such as polyneuropathy.2
Accumulating evidence has suggested that zeolites may significantly affect the regulation of the immune system. Ueki et al have reported that silica, silicates, and aluminosilicates may act as nonspecific immunostimulators in a manner similar to that of the superantigens (SAgs),16, 17 a class of powerful, immunostimulatory bacterial and viral toxins that are able to cause a number of diseases characterized by fever and shock. Unlike conventional antigens, SAgs bind as unprocessed proteins to particular motifs of the variable region of the β chain (Vβ) of the T-cell receptor (TcR) outside the antigen-binding groove and to invariant regions of major histocompatibility complex (MHC) class II molecules on the surface of antigen-presenting cells (APCs). As a consequence, SAgs, in nanogram to picogram concentrations, stimulate up to 10% to 30% of the host T-cell repertoire, whereas in conventional antigenic peptide-TcR binding, only 1 in 105 to 106 T cells (0.01%-0.0001%) is activated.18 In accordance with this theory, proinflammatory macrophages, which belong to MHC class II APCs, are activated by fibrogenic silicate particles,19, 20 and the removal of MHC class II DP/DR+ cells results in a lack of macrophage stimulation by the silicate chrysotile.16 More recently, Pavelic et al have demonstrated that the lymphocytes from lymph nodes of mice that were fed for 28 days with micronized zeolite clinoptilolite provoked a significantly higher allogeneic graft-versus-host reaction than did lymphocytes in control mice. After the mice were administered clinoptilolite intraperitoneally, the number of peritoneal macrophages increased significantly, as did their superoxide anion production.21
The significant immunostimulatory properties of natural zeolites, as described in these in vitro and animal studies, suggest that zeolite may provide clinical benefits as an oral dietary supplement. This study is the first to evaluate the impact of dietary supplements containing the natural zeolite clinoptilolite on the immune system of patients who demonstrate immunodeficiency.MATERIALS AND METHODS
Study Population
Adult outpatients suffering from primary or secondary immunodeficiency were eligible for participation in this prospective, open, and controlled parallel-group observational study. Nine primary care physicians in the greater Neubrandenburg area in Germany participated as investigators and recruited patients frequenting their private practice for the treatment of known immunodeficiency, determined in each case on the basis of clinical symptomatology (such as recurrent infections and autoimmune disorders) and pathologic lymphocyte counts.Interventions
The dietary supplements administered in this study consisted of Megamin® 500 mg and Lycopenomin® 500 mg (both manufactured by Tribomin d.o.o., Osijek, Croatia), which were provided by Megamin GmbH, Berlin, Germany. The primary ingredient in both products is TMAZ® (Tribomin d.o.o.), a tribomechanically activated version of the natural zeolite clinoptilolite (Table 1). Each 500-mg Megamin capsule also contains 87 mg of dolomite (CaMg(CO3)2), and each 500-mg Lycopenomin capsule contains several antioxidants, including 75 mg of vitamin C, 50 mg of natural tomato-derived lycopene, 50 mg of tomato powder, 25 mg of grape seed extract, and 2 mg of plantderived magnesium stearate.
During a 6- to 8-week period, eligible patients received, depending on the severity of their immunodeficiency, either 4 Megamin capsules or 2 Lycopenomin capsules three times a day. Patients with more severe immunodeficiency were given Lycopenomin, since this product was anticipated to be the more powerful antioxidant. All other medical therapies intended to treat the immunodeficiency disorder were to be continued unchanged throughout the study.
*Analysis by ISEGA Forschungs- und Untersuchungsgesellschaft mbH, Aschaffenburg, Germany
Table 1. Composition and Physicochemical Properties of the Tribomechanically Activated Zeolite
Clinoptilolite (TMAZ®)*
Chemical composition SiO2, 65.0-71.3%; Al2O3, 11.5-13.1%; CaO 2.7-5.2%; K2O, 2.2-3.4%; Fe2O3, 0.7-1.9%; MgO, 0.6-1.2%; Na2O, 0.2-1.3%; TiO2, 0.1-0.3%; Si/Al ratio, 4.8-5.4 Empirical formula (Ca,K2,Na2,Mg)4Al8Si40O9696 × 24H2O Physicomechanical properties Specific mass, 2.2-2.5 g/cm3; porosity, 32-40%; effective pore diameter, 0.4 nm Ion-exchanging capacity Total exchange capacity, 1.2-1.5 mol/kg; Ca2+, 0.64-0.98 mol/kg; Mg2+, 0.06-0.19 mol/kg; K+, 0.22-0.45 mol/kg; Na+, 0.01-0.19 mol/kg Ion-exchanging selectivity Cs>NH4 +>Pb2+>K+>Na+>Mg2+>Ba2+>Cu2+>Zn2+ Chemicals absorbed NH3, hydrocarbons C1-C4, CO2, H2S, SO2, NOx, aldehydes Toxicity Toxicity Nontoxic; generally recognized as safe (GRAS) according to US Code of Federal Regulations (21 CFR 182, Subpart C) Laboratory Measurements
To evaluate changes in the status of the immune system, blood and lymphocyte counts were obtained at baseline and after about 6 weeks of supplementation therapy, each time within the framework of routine laboratory assessments. Routine visits took place about twice monthly. All laboratory assessments were established in accordance with the Guidelines of the German National Medical Council (Bundesärztekammer) at the Laboratory for Immunology, Neubrandenburg, Germany. Blood samples were obtained routinely with an EDTAS-Monovette® 2.7 mL (Sarstedt AG & Co., Nümbrecht, Germany) between 12 and 1 PM to avoid variation due to circadian rhythm. Blood counts were performed with an automated blood counting machine (Sysmex Corporation, Kobe, Japan). Monoclonal antibodies (Beckman Coulter, Inc., Fullerton, California) in conjunction with flow cytometry (FACScanIM Becton, Dickinson and Co., San Jose, California) were used for the quantitative analysis of several lymphocyte subsets in erythrocyte-lysed whole blood, including mature B lymphocytes (CD19+), mature T lymphocytes (CD3+), T-helper cells (CD3+/CD4+), T-suppressor/cytotoxic cells (CD3+/CD8+), activated T lymphocytes (CD3+/HLA-DR+), and natural killer (NK) cells (CD56+).Statistical Analysis
Owing to the explorative character of the study and because multiple testing was performed without adjustment for type 1 error, all statistics reported in this study are interpreted descriptively. The statistical significance was set to P<.01 for treatment effects within groups. In addition to the standard methods used for reporting descriptive statistics, nonparametric tests such as the ÷2 test, Wilcoxon test, and Mann- Whitney-U test were applied to assess treatment effects within groups and differences between groups. Between-group comparisons were based on the change from baseline values of variables to adjust for potential baseline differences between groups.RESULTS
A total of 65 patients with a diagnosis of immunodeficiency participated in the trial. Four patients withdrew prematurely and were not included in the analysis. Thus, 61 subjects formed the primary analysis sample, 31 of whom received Megamin and 30 Lycopenomin.
Both groups had similar baseline characteristics (Table 2) except for the white blood cell count, which was lower in patients given Lycopenomin; this was expected, as these patients had the more severe immunodeficiency disorders (Tables 3 and 4).
Values are expressed as number (%) unless otherwise noted.
Table 2. Baseline Data of the Treatment Groups Megamin Lycopenomin Total (n=31) (n=30) (n=61) P value* Sex Male 9 (29.0) 7 (23.3) 16 (26.2) Female 22 (71.0) 23 (76.7) 45 (73.8) .77 Age, mean yr ± SD 56±14 60±13 58±14 .29 Duration of treatment,
mean days ± SD57±16 49±6 53±13 .06 Disorder .12 Unspecified immunodeficiency 26 (83.9) 18 (60.0) 44 (72.1) Cancer 3 (9.7) 7 (23.3) 10 (16.4) Type I allergy 1 (3.2) 3 (10.0) 4 (6.6) Rheumatoid arthritis 0 1 (3.3) 1 (1.6) Furuncles 1 (3.2) 0 1 (1.6) Viral infection 0 1 (3.3) 1 (1.6)
*χ2 test for binomial data, and Mann-Whitney-U test for continuous data.
Table 3. Blood Counts Before and After Supplementation
With Megamin® and Lycopenomin®Normal Megamin (n=31) Lycopenomin (n=30) Change Between Blood Count* Range Baseline Final P value* Baseline Final P value* Groups, P value* Hb, mmol/L 7-10 8.4 8.4 .62 8.3 8.2 .46 .70 (7.8-8.9) (7.7-9.1) (7.3-8.7) (7.5-8.9) Hc, % 35-50 40 41 .09 40 40 .31 .54 (39-43) (38-44) (37-42) (36-43) WBC, Gpt/L 4-10 6.60 6.30 .11 5.70 5.35 .03 .70 (5.60-7.50) (5.25-7.20) (4.80-7.10) (4.13-6.25) PLT, Gpt/L 100-350 234 243 .33 222 209 .99 .53 (197-264) (197-262) (176-258) (190-259) RBC,Tpt/L 4-5 4.50 4.60 .26 4.35 4.35 .89 .52 (4.25-4.85) (4.25-4.80) (4.13-4.70) (4.03-4.68) MCH, fmol/L 1.6-1.9 1.90 1.90 .73 1.80 1.90 .48 .29 (1.80-1.90) (1.80-1.90) (1.80-1.90) (1.80-1.90) MCHC, mmol/L 20.0-22.5 20.6 20.4 .08 20.5 20.5 .20 .87 (20.4-21.0) (20.0-20.9) (19.9-21.0) (19.9-20.9) MCV, fL 85-95 90.0 91.0 .09 91.0 91.0 .004 .46 (86.5-93.5) (87.5-93.5) (87.3-93.0) (88.3-93.0) Values are given as medians (percentiles 25-75). Between-group comparisons analyzed baseline-final differences.
*Within group comparisons: Wilcoxon test; between groups comparisons: Mann-Whitney-U test
Hb=hemoglobin; Hc=hematocrit; WBC=white blood cells; PLT==platelets; RBC=red blood cells; MCH=mean corpuscular Hb;
MCHC=mean corpuscular Hb concentration; MCV==mean corpuscular volume.
Table 4. Relative and Absolute Lymphocyte Counts Before and After Supplementation with Megamin®
and Lycopenomin®
Lymphocyte Normal Megamin (n=31) Lycopenomin (n=30) Change Between Count* Range Baseline Final P value* Baseline Final P value* Groups, P value* Total,Gpt/L 1.0-3.6 1.73
(1.57-2.02)1.78
(1.39-2.17).74 1.11
(0.85-1.54)1.13
(0.95-1.43).59 .45 CD3+, % 62-86 67.0
(60.5-72.5)69.0
(61.0-75.0).03 65.0
(56.3-72.5)65.5
(613-77.8).005 .62 CD19+, % 7-23 10.0
(8.0-14.0)12.0
(10.0-14.0).009 10.0
(7.0-14.0)10.0
(8.0-14.8).27 .17 CD4+, % 31-59 41.0
(35.0-52.0)44.0
(39.5-52.0).008 41.5
(35.0- 49.0)43.5
(38.3-50.0).02 .99 CD8+, % 19- 48 23.0
(18.5-31 .5)24.0
(18.5-31.5).32 22.0
(17.0-33.5)21.0
(17.3-33.0).23 .94 CD4+/CD8+ 0.9- 1 .8 1.60
(1.20-2.85)1.70
(1.40- 2.75).37 2.10
(1.20-2.80)2.0
(1.13-2.75).48 .82 HLA-DR+, % 9-16 9.0
(8.0- 13.0)10.0
(8.0-15.5).002 12.0
(8.0-1 7.8)10.0
(8.3-16.0).64 .02 CD56+, % 5-26 25.0
(19.0-31.5)22.0
(22.0-43.0).008 27.5
(16.8-35.3)20.5
(16.5-28.3).005 .42 CD3+/ cells/μl 1200-1790 1343
(1074-1590)1383
(1252-1700).06 871
(683-1108)974
(789-1177).13 .84 CD19+, cells/μl 150-480 227
(124-304)243
(172-359).005 134
(80-249)156
(100-266).24 .14 CD4+, cells/μl 590-1200 825
(682-1072)950
(740-1099).05 543
(410-836)589
(500-812).03 .78 CD8+, cells/μl 400-1010 450
(361-602)446
(383-638).09 329
(223-400)359
(268-419).63 .39 HLA-DR+, cells/μl 40-300 209
(163-243)222
(171-322).01 179
(137-206)163
(116-234).77 .02 CD56+, cells/μl 110-550 512
(390- 599)430
(337-615).08 363
(263-546)354
(188-504).005 .55 Values are given as medians (percentiles 25-75). Between-group comparisons analyzed baseline-final differences.
*Within group comparisons: Wilcoxon test; between groups comparisons: Mann-Whitney-U-test.
CD=Clusters of Differentition; HLA=Human Leukocyte AntigenSix to 8 weeks of supplementation therapy did not relevantly affect the blood counts in either of the 2 treatment groups (Table 3). Among patients given Megamin, the CD4+, CD19+, and HLA-DR+ lymphocyte counts were significantly increased over baseline values, whereas the CD56+ cell count was significantly decreased. Among those given Lycopenomin, the CD3+ cell count was significantly increased over baseline and the CD56+ lymphocyte count was also significantly decreased. In general, the relative lymphocyte counts corresponded with the absolute cell counts (Table 4).
No adverse reactions to treatments were observed.DISCUSSION
To our knowledge, this is the first prospective clinical study of the effects of oral supplementation with the natural zeolite clinoptilolite on the immune system of patients with an immunodeficiency disorder. In this population, 6 to 8 weeks of therapy did not cause relevant changes in blood counts. This finding is in accordance with data from a toxicology study in which mice had been fed a clinoptilolite-rich diet for 6 months.22 Indeed, clinoptilolite supplementation produced significant and relevant increases in the B lymphocyte (CD19+), T-helper cell (CD4+), activated T lymphocyte (HLA-DR+), and, to a lesser extent, total T lymphocyte (CD3+) counts and decreases in the NK cell (CD56+) count. The clinical relevance of these findings is supported by the improved well being reported by the patients (data not shown) who underwent clinoptilolite supplementation therapy. The effects of supplementation, particularly on the activated T lymphocyte count, were more pronounced in the Megamin group than in the Lycopenomin group.
Patients given Lycopenomin exhibited significantly lower total lymphocyte counts at baseline than did patients given Megamin, which is why they were assigned the more powerful antioxidant. The TMAZ doses administered with Megamin were three times higher than those taken with Lycopenomin (3.6 vs 1.2 g daily). Hence, the more pronounced effects in the Megamin group may be attributed to a dose-response relationship of the zeolite, although the results are not adjusted for baseline differences in severity of illness between groups. In addition, the contribution of Lycopenomin's other antioxidants to the net effects was not addressed or examined. Moreover, it remains unclear whether 6 to 8 weeks of treatment is sufficient to achieve the maximal effect. The results of other studies that have investigated drug-induced immunomodulation suggest that more-significant effects may be realized beyond two months of treatment.23 Thus, future studies should include a 4- to 6-month treatment period and employ repeated measurements.
In this study, because the patient population did not alter their primary therapy for the treatment of their immunodeficiency disorder, the observed treatment effects can likely be attributed to the Megamin and Lycopenomin supplements. Although no adjustments were made for type 1 error, the number of statistically significant test results suggests these effects are beyond chance. Obviously, these effects must be examined further in a suitably sized, randomized placebo-controlled trial.
Although an immunomodulatory effect of natural zeolite has been clinically demonstrated, its mode of action must still be elucidated. After ingestion, clinoptilolite is resistant to degradation by gastric and intestinal juices, and its major constitutive elements are not significantly absorbed from the gut into systemic circulation. No traces of silicon have been detected in the serum of Wistar rats or CBA mice fed with clinoptilolite. Zeolite particles, however, have been found in the first and second layers of duodenal cells.2 The interaction of orally administered zeolite particles with mucosal associated intestinal lymphoid tissue may trigger an immune response similar to the one observed after the intraperitoneal administration of micronized zeolite. In both cases, the number of peritoneal macrophages, as well as their superoxide anion (O2-) production, is increased, while NO production is decreased.21 Resident macrophages in the airways and alveolar spaces have also been observed to release reactive oxygen species, such as O2-, after phagocytosis of inhaled silica particles. Reactive oxygen species have been found to be important second messengers for signal transduction in general,24 and alterations in the redox homeostasis of cells may play an important role in modulating immune functions. For example, transmembrane redox signaling activates nuclear factor kappa B (NFκB) in macrophages and T lymphocytes.25,26 NFκB is involved in the activation of a large number of genes in response to inflammation, viral and bacterial infections, and other stressful conditions that necessitate rapid reprogramming of gene expression.
In addition, direct interactions of silicate particles with alveolar cells have been observed that may enhance the understanding of the immunostimulation provided by orally administrated zeolite. It seems that mineral particles can trigger alterations in gene expression by initiating signaling events upstream of gene transactivation.27 The exposure of alveolar macrophages to silicate particles can also activate mitogenactivated protein kinases, stress-activated protein kinase, and protein kinase C.28 Important transcription factors such as activator protein 1 and NFκB are also activated, and the expression of proinflammatory cytokines such as interleukin 1α, interleukin 6, and TNF-α is enhanced.29
Macrophage activation and the subsequent initiation of intracellular signaling pathways, together with the polyclonal human T-lymphocyte activation observed in vitro, have led to the hypothesis that silicate particles act as SAgs.16 If this hypothesis can be confirmed, dietary supplementation with natural zeolites holds promise in the treatment of autoimmune disorders and infectious and malignant diseases, the pathogenesis of which is linked to the action of SAgs.30-32 Zeolite supplementation therapy has demonstrated other antitumor effects in in vitro and animal studies and may prove beneficial as an adjunct to cancer therapy.33,34CONCLUSION
Accumulating evidence from preclinical studies and the first human trials suggests oral zeolite supplementation therapy is associated with significant immunomodulatory effects that can enhance the primary treatment of a variety of immunodeficiency disorders. Further research is necessary to clarify the proposed mechanisms of action of the zeolite compounds and to confirm the promising results observed in this pilot study.
REFERENCES
- Mumpton FA. La roca magica: uses of natural zeolites in agriculture and industry. Proc Natl Acad Sci USA. 1999;96:3463-3470.
- Pavelic K, Hadzija M. Medical applications of zeolites. In: Auerbach SM, Carrado KA, Dutta PK (eds). Handbook of Zeolite Science and Technology. New York: Dekker; 2003; pp 1143-1174.
- Cattaneo MV, Chang TM. The potential of a microencapsulated urease-zeolite oral sorbent for the removal of urea in uremia. ASAIO Trans. 1991;37:80-87.
- Patzer JF II, Yao SJ, Wolfson SK Jr. Zeolitic ammonium ion exchange for portable hemodialysis dialysate regeneration. ASAIO J. 1995;41:221-226.
- Seidel H, Bartko P, Kovác G, Paulíková I, Nagy O. Effects of haemoperfusion on selected Indices of blood biochemistry in sheep. Acta vet Brno. 1997;66:213-218.
- Rodriguez-Fuentes G, Barrios MA, Iraizoz A, Perdomo I, Cedre B. Enterex-anti-diarrheic drug based on purified natural clinoptilolite. Zeolites. 1997;19:441-448.
- Young SW, Qing F, Rubin D, et al. Gadolinium zeolite as an oral contrast agent for magnetic resonance imaging. J Magn Reson Imaging. 1995;5:499-508.
- Keeting PE, Oursler MJ, Wiegand KE, Bonde SK, Spelsberg TC, Riggs BL. Zeolite A increases proliferation, differentiation, and transforming growth factor beta production in normal adult human osteoblast-like cells in vitro. J Bone Miner Res. 1992;7:1281-1289.
- Ivkovic S, Zabcic D. The effect of tribomechanically activated zeolite (TMAZ) on total antioxidant status of healthy individuals and patients with malignant disease. Free Radic Biol Med. 2002; 33(suppl 1):172.
- Ivkovic S, Zabcic D. Antioxidative Therapy: nanotechnology product TMA-Zeolite reduces oxidative stress in cancer and diabetic patients. Free Radic Biol Med. 2002;33(suppl 2):331.
- Nikawa H, Yamamoto T, Hamada T, Rahardjo MB, Murata H, Nakanoda S. Antifungal effect of zeolite-incorporated tissue conditioner against Candida albicans growth and/or acid production. J Oral Rehabil. 1997;24:350-357.
- Morishita M, Miyagi M, Yamasaki Y, Tsuruda K, Kawahara K, Iwamoto Y. Pilot study on the effect of a mouthrinse containing silver zeolite on plaque formation. J Clin Dent. 1998;9:94-96.
- Uchida T, Maru N, Furuhata M, et al. [Anti-bacterial zeolite balloon catheter and its potential for urinary tract infection control.] Article in Japanese. Hinyokika Kiyo. 1992;38:973-978.
- Oschilewski U, Kiesel U, Kolb H. Administration of silica prevents diabetes in BB-rats. Diabetes. 1985;34:197-199.
- Charlton B, Bacelj A, Mandel TE. Administration of silica particles or anti-Lyt2 antibody prevents beta-cell destruction in NOD mice given cyclophosphamide. Diabetes. 1988;37:930-935.
- Ueki A, Yamaguchi M, Ueki H, et al. Polyclonal human T-cell activation by silicate in vitro. Immunology. 1994;82:332-335.
- Aikoh T, Tomokuni A, Matsukii T, et al. Activation-induced cell death in human peripheral blood lymphocytes after stimulation with silicate in vitro. Int J Oncol. 1998;12:1355-1359.
- Muller-Alouf H, Carnoy C, Simonet M, Alouf JE. Superantigen bacterial toxins: state of the art. Toxicon. 2001;39:1691-1701.
- Allison AC, Harington JS, Birbeck M. An examination of the cytotoxic effects of silica on macrophages. J Exp Med. 1966;124:141-154.
- Drumm K, Oettinger R, Smolarski R, Bay M, Kienast K. In vitro study of human alveolar macrophages inflammatory mediator transcriptions and releases induced by soot FR 101, Printex 90, titandioxide and Chrysotile B. Eur J Med Res. 1998;3:432-438.
- Pavelic K, Katic M, Sverko V, et al. Immunostimulatory effect of natural clinoptilolite as a possible mechanism of its antimetastatic ability. J Cancer Res Clin Oncol. 2002;128:37-44.
- Martin-Kleiner I, Flegar-Mestric Z, Zadro R, et al. The effect of the zeolite clinoptilolite on serum chemistry and hematopoiesis in mice. Food Chem Toxicol. 2001;39:717-727.
- Nezhinskaia GI, Sapronov NS. [Assessment of the rhythm of lymphocyte stimulation and suppression as a criterion of prognosis of the effects of immunomodulatory drugs.] Article in Russian. Patol Fiziol Eksp Ter. 2002;3:22-25.
- Martin LD, Krunkosky TM, Dye JA, et al. The role of reactive oxygen and nitrogen species in the response of airway epithelium to particulates. Environ Health Perspect. 1997;105(suppl 5): 1301-1307.
- Ginn-Pease ME, Whisler RL. Redox signals and NF-kappaB activation in T cells. Free Radic Biol Med. 1998;25:346-361.
- Kaul N, Choi J, Forman HJ. Transmembrane redox signaling activates NF-kappaB in macrophages. Free Radic Biol Med. 1998;24:202-207.
- Tsuda T, Morimoto Y, Yamato H, et al. Effects of mineral fibers on the expression of genes whose product may play a role in fiber pathogenesis. Environ Health Perspect. 1997;105(suppl 5):1173-1178.
- Lim Y, Kim SH, Kim KA, Oh MW, Lee KH. Involvement of protein kinase C, phospholipase C, and protein tyrosine kinase pathways in oxygen radical generation by asbestos-stimulated alveolar macrophage. Environ Health Perspect. 1997;105(suppl 5):1325-1327.
- Simeonova PP, Toriumi W, Kommineni C, et al. Molecular regulation of IL-6 activation by asbestos in lung epithelial cells: role of reactive oxygen species. J Immunol. 1997;159:3921-3928.
- Totterman TH, Gidlof C, Ragnarsson L, et al. Targeted superantigens for immunotherapy of haematopoietic tumours. Vox Sang. 1998;74(suppl 2):483-487.
- Macphail S. Superantigens: mechanisms by which they may induce, exacerbate and control autoimmune diseases. Int Rev Immunol. 1999;18:141-180.
- Stevens DL. Superantigens: their role in infectious diseases. Immunol Invest. 1997;26:275-281.
- Zarkovic N, Zarkovic K, Kralj M, et al. Anticancer and antioxidative effects of micronized zeolite clinoptilolite. Anticancer Res. 2003;23:1589-1595.
- Pavelic K, Katic M, Sverko V, et al. Immunostimulatory effect of natural clinoptilolite as a possible mechanism of its antimetastatic ability. J Cancer Res Clin Oncol. 2002;128:37-44.